Foot arches are fundamental to optimal physical health. The arches act in two main capacities, firstly to act as a shock absorber (being adaptive and bendy) and secondly to act as a lever (stiff and resilient) for locomotion. There are vast differences in foot “Types”. This is dependent on a number of factors such as bone structure, ligamentous elasticity and myofascial function and balance. The foot “Types” are usually classed as pronators (Medially tilted) or supinators (Laterally tilted). This typing must be considered in both dynamic and static postures and also given close consideration as to the overall posture of the leg, pelvis and spine. This typing must be considered as a plastic property and manipulable to achieve functional balance of the foot and its arches. This essay will discuss the arches and the main tendons influencing their function. Clinical relevance to tendon and fascial length/tension relationship will be proposed.
Neurologically the foot is held in high regard by the sensory and motor homunculus with around one quarter of its capacity devoted to the foot.
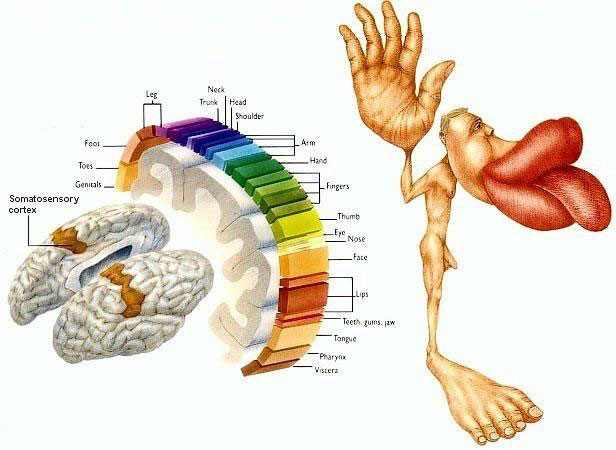
Clinically the foot is considered a major control platform and imbalance in this area has far reaching physical and neurological effect. Some practitioners class the foot and the jaw as the “bookends” of postural stability.
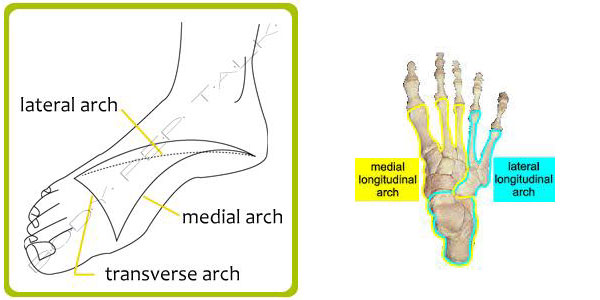
The foot as a proprioceptive base consists of three arches. 1.The medial longitudinal arch: 2. The Lateral longitudinal arch: 3. the Transverse arch.
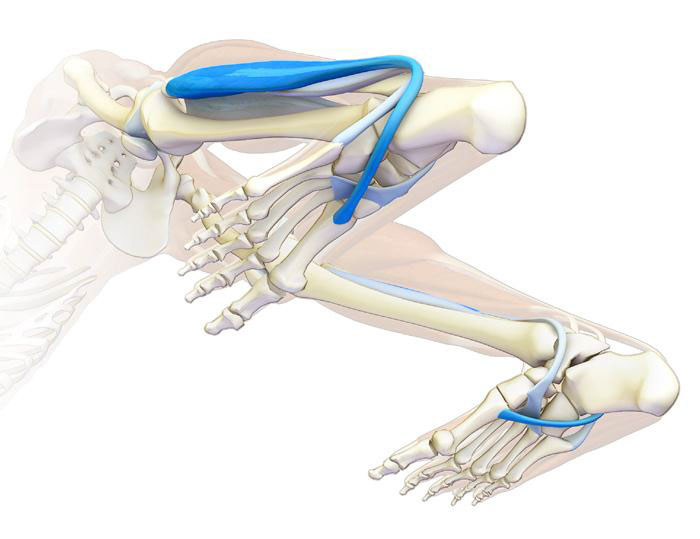
This rather complex relationship between the very congruent bones of the foot is wonderfully supported by the tendons of the lower leg. Thomas Myers describes this as a “stirrup” of myofascia that supports the arches.
This stirrup consists of two muscles that pass around the mid foot and form a fascial continuum. The Tibialis anterior passes down the anterior compartment of the shin over the navicular (medially) and attaches to the joint capsule between the first cuneiform and the first metatarsal. The peroneus longus tendon attaches to the same cuneiform and forms a direct connection to the lateral aspect of the foot, ankle joint and lateral compartment of the shin as it extends up to the head of the fibula. This loop is described By Tom Myers as a myofascial sling named the Spiral Line.
For the foot arches to be resilient and adaptable these myofascial elements are of prime importance. Shortening of the Peroneus Longus tendon will tend to tip the foot into a pronation (medially rotated) pattern. This would see the tibialis anterior in a locked long position. The navicular would medially tilt and the medial arch lengthens. Conversely a foot that tends toward a supination (laterally rotated) pattern would see the tibialis anterior locked short and the peroneus longus locked long.
In my opinion these two muscles are the most significant in supporting the arches of the foot but there are (at least) three more that influence the foot’s arches structure and balance.
Flexor hallucis longus muscle (FHL) is one of the three deep muscles of the posterior compartment of the leg that distally attaches to the plantar surface of the hallux (great or big toe). Although this muscle attaches distal to traditional bones of the medial arch I believe it has a great role in stabilising the ball of the foot. If there is inhibition or dysfunction in this muscle, plantar flexion at the front of the arch is lost, the arch may lengthen. This is evident at toe off and may create a “medial whip “of the calcaneus, loss of hip extension and shortening of the lateral compartment. Myofascial stimulation is recommended and or placing a thin wedge of cork under the first ray to stimulate a stronger plantar flexion action during walking.
The Tibialis anterior has a strong action on the medial arch. The tibialis posterior muscle descends posterior to the medial malleolus and inserts into the bases of the second, third and fourth metatarsals, the second and third cuneiforms and the cuboid. The main portion inserts into the tuberosity of the navicular and the plantar surface of the first cuneiform. The tibialis posterior contracts to produce inversion and assists in the plantar flexion of the foot at the ankle. The tibialis posterior has a major role in supporting the medial arch of the foot. Dysfunction of the tibialis posterior, including rupture of the tibialis posterior tendon, can lengthen the medial arch.
Peroneus brevis is a small muscle with a significant role in supporting the lateral arch. It arises from the lower two-thirds of the lateral surface of the body of the fibula, medial to the peroneus longus. It attaches to the base of the fifth metatarsal. It is prone to fibrosis following ankle sprains and if it loses length will prevent the foot from lateral rotation and a shortening of the lateral arch (pronation).
Myofascial integration of the foot arches clearly has long reaching effects on the overall postural balance of the system.
Click here to contact us about our Myofascial services or email on [email protected] or call on 02 9817 1781.